- Introduction
- Useful People to Know and Knowing Their Roles.
- ACCS Training Programme Directors:
- Training Leads at Individual Trusts:
- A Note on Clinical Supervision
- General Overview
- Preparing For ACCS
- Teaching During ACCS For Anaesthetists
- Year 1 – No specific anaesthesia teaching…
- Year 2 – Getting your IAC, learning for the Primary FRCA and understanding critical care concepts.
- Year 3 – Consolidating anaesthetic practise, gaining independence, obtaining the Primary FRCA, branching out into other areas. Readying for specialist applications
- Portfolio, ARCP and Maximising WBPAs
Introduction
ACCS (Acute Common Care Stem) Training is a challenging but extremely rewarding pathway into higher training for doctors interested in emergency medicine, acute medicine, anaesthetics and intensive care medicine alike. It also has major advantages specifically if you are focussed on a career in ICM as it acknowledges training in the other disciplines at a later stage, so you don’t have to leave your base specialty in your final years for up to six months, for example returning to acute medicine if you have completed core anaesthetic training.
Moreover and speaking from experience though, it gives you an appreciation of the other specialties’ workloads and skillsets. This can be vital as an anaesthetist as it fosters more positive working relationships between colleagues, more timely recognition of problems, diagnosis and treatment and I believe can have a major impact on acute and emergency patient care and flow from emergency department through the hospital.
However, like with any training pathway there can be ambiguities, uncertainties and questions along the way which this guide aims to address. I’d like to stress this guide is biased towards anaesthetic training and the requirements you should expect to have each year up until the point of completing CT3 (i.e. the full three years of the programme).
Perhaps most importantly though, there are changes due to happen in 2021 to the ACCS and core anaesthesia curriculums and this guide will be updated to reflect this in due course with potentially large changes in the amount and style of WBPAs needed. In the meantime, I hope it is useful for those on the existing curriculum, even if it just helps to organise your thinking a bit!
Please don’t hesitate to get in touch with me on d.cegielski@doctors.net.uk if you have any further queries about experiencing the programme as a trainee or if you would like any of the template logbooks later on in the guide!
Congratulations on your appointment and all the best with your training!
Authored by: Dr David Cegielski (Consultant Anaesthesia)
Useful People to Know and Knowing Their Roles.
There will be various points during your training where you want to speak to a supervisor, or a programme lead about certain aspects of the curriculum, signoffs and teaching dates. Below is a list of some key names that are all very approachable if you have questions and what they are responsible for:
ACCS Training Programme Directors:
Region | Name | Job Specialty | Email |
North West | Jon Argall | Emergency Medicine | |
Mersey | Tim Wharton | Emergency Medicine |
Training Leads at Individual Trusts:
As you can see there are a variety of specialties for the training leads which can influence your experience as an anaesthetic trainee. It is possible that they will be your educational supervisor for the duration of the first two years as well so they will know what is required of you in terms of WBPA sign offs at various stages. The leads at each hospital are:
Name | Location | Job Specialty | Email |
Argall, Jon | Blackpool | EM | |
Baird, Sarah | Whiston | ||
Barrie, Janet | Pennine ACCS | Anaesthesia | |
Brooks, Neil | Leighton | Anaesthesia | |
Butler, John | MRI | EM/ICM | |
Clarke, Tim | Blackburn | Anaesthesia | |
Cockerham, Rowena | MRI/Trafford | Anaesthesia | |
Evans, Louise | Stockport | Anaesthesia | |
Goddard, Chris | Southport & Ormskirk | Anaesthesia/ICM | |
Gotz, Vera | Lancaster | AM/ICM | |
Holzmann, Tim | AM Representative | AM/ICM | |
Jumani, Deepa | Warrington | Anaesthesia | |
McGrattan, Ken | Preston | Anaesthesia/ICM | |
Mittal, Rajnish | Countess of Chester | EM | |
Mohanraj, Arun | Wigan | Anaesthesia | |
Newton, Phillipa | UHSM Lead | AM | |
Nicol, Mark | Macclefield | EM | |
O'leary, Clare | St Helens | EM | |
Parkinson, Elizabeth | Wirral | EM | |
Protheroe, Richard | Salford | Anaesthesia/ICM | |
Roberts, Cath | Preston | EM/ICM | |
Williams, Cath | Bolton | EM |
A Note on Clinical Supervision
It’s important to remember that whilst the consultants above are responsible for your training in ACCS whilst at their hospital, this often covers the first two years. Each placement will usually have a nominal clinical supervisor that isn’t the same for each trainee rotating through. There have been reports where trainees have arrived for placements and have not been allocated a clinical supervisor and they don’t know the objectives of an ACCS portfolio. I would strongly advise to report this to the training lead at your trust so that they can bring the clinical supervisor up to speed on your needs but also ensure they are delivering the education you should be getting.
To avoid this, ideally a month before starting your 6-month block, try to find out who your clinical supervisor will be and ensure they know what you need from your training and arrange to meet them early. If you write a personal development plan with your goals (see later section) then you can use this as your educational contract with that supervisor to evaluate their supervision too.
General Overview
The three-year programme is divided up in the North West as usually as Years 1 and 2 at the same base hospital, then year 3 at a different centre. Normally this follows the pattern of Teaching Hospital then District General Hospital or vice-versa as follows:
Year 1 – CT1 ACCS |
6 months | 6 months |
Emergency Medicine | Acute Medicine |
I.e. The non-anaesthetics year. However, as shown later, it’s imperative to keep up to date with your portfolio and upload assessments to the lifelong learning platform. You have no commitments to anaesthetic teaching in this year.
Year 2 – CT2 ACCS |
6 months | 6 months |
Anaesthetics (Including IAC) | Intensive Care Medicine |
I.e. Treat this as your “old-style” CT1 Anaesthetic year. With the new anaesthetic curriculum coming in, it will be hard not to draw comparisons when you see somebody who is CT2 Anaesthetics with an IAC and a year of cases under their belt compared to a CT2 ACCS who is starting anaesthetics for the first time and have to catch up with the primary FRCA knowledge. This is part of the reason for aligning the years of training at core level so as to provide sufficient anaesthetic experience to both cohorts in readiness for what will be ST4 as well as allow additional time for the primary FRCA to be obtained.
Year 3 – CT3 ACCS |
12 Months |
Anaesthetics (Including IAC Obstetrics and completion of Basic Training) |
I.e. the old style CT2 Anaesthetics year. A full year to focus on anaesthesia, consolidate knowledge and skills for the primary FRCA whilst colleagues at CT3 anaesthesia may be catching up on ICM/Obstetric/other experience. This aims to even out anaesthesia exposure between core and ACCS but also provides the foundation for application for ICM.
Preparing For ACCS
There are a few important things to do before or during the first few weeks of ACCS training, regardless of what your first placement is:
- Organise a meeting/talk with your educational and clinical supervisors and establish
- Where to go on the first day
- What the objectives are of the placement
- Rota/roles/responsibilities
- Personal Development plan – and plan your assessments per week/month
- Make sure they know you are Anaesthesia badged but won’t affect what work you undertake with them – this will hopefully help them focus on what assessments you may be better doing during their rotation.
- Register for membership with the RCOA and Lifelong Learning (LLL) from the beginning of CT1
- Join the AAGBI – not the most pressing issue now, but if you end up doing any transfers in CT2, they provide free indemnity for any accident whereby you may get hurt in a transfer, the MDU/MPS/BMA/GMC don’t!
- Produce your own logbook:
- Doesn’t have to be an exhaustive list, but you can make a simple Excel spreadsheet/word document (see Appendix 1) that can record cases your see, your involvement, any procedures done and perhaps most importantly to overcome the niggles of LLL, map this to the curriculum and any WBPAs you’ve done.
- Make a document of online teaching you’ve completed and again map it to presentations in the curriculum.
- Gets you into the habit of what you’ll be doing in CT2 for anaesthetics and for the ICM placement – some supervisors like to see what exposure you’ve had to certain aspects of the curriculum alongside WBPAs
- Set a precedent for good record keeping, for some higher modules in your training; supervisors like case-specific logbooks (e.g. Neuroanaesthesia).
- Planning for CT2 – sounds ridiculous but you’ll have colleagues sitting the exam when you haven’t done any anaesthesia at all in CT2. Have a think about when to start the groundwork and it’s worth getting some early reading in.
- Organise your study leave for regional teaching (see separate section)
- Enrol on ALS (if not already done one in foundation)/APLS/ETC/ATLS courses. They are a huge help during medicine and A&E rotations since you’ll often be part and lead an arrest team – good sign off opportunities.
- Sign up for:
- St Emlyns Online Classroom – a great resource and forum with a separate area for North West Trainees. At Wythenshawe (now MFT) we were expected to work through and complete all the modules by the end of the six months in A&E. (http://classroom.stemlyns.org.uk/login/index.php).
- E-Learning for Healthcare, a fantastic learning resource for anaesthesia at any stage complete with curriculum mapped topics and MCQs for the primary FRCA but also has the entire emergency medicine curriculum mapped on there too to support Dr Argall’s days (portal.e-lfh.org.uk).
Teaching During ACCS For Anaesthetists
This has been a source of confusion in the past, but if you are organised, request study leave well in advance and perhaps most importantly inform your rota masters and tutors what you need to attend, then you can acquire a lot of CPD over the year as well as fulfil the mandatory training requirements.
Year 1 – No specific anaesthesia teaching…
Main Objectives:
- Gain an increasing understanding in handling acute medical and emergency department presentations and also understand the evidence base behind what you’re diagnosing and treating.
- Construct a core medical and surgical framework underpinning the first year of ACCS
- Promote your confidence in assessing and treating patients more independently with local supervision
Expected Teaching to Attend:
- Dr Argall’s Regional Teaching Days – happen every two months and usually have a theme attached to each (e.g. cardiovascular, respiratory, neurological). At the moment they are virtual but be prepared to participate as it’s far from didactic teaching involving group work, evidence reviews, etc. Outside of a pandemic they usually take place in Blackpool Victoria Hospital in the Education Centre.
- Simulation Day(s) – You’ll be contacted about which date you’ll be attending and like other simulation teaching they focus on some of the major and acute presentations – great opportunity to sign off and volunteer for ones you haven’t seen at work!
- Local Teaching – As Anaesthesia badged you don’t have any obligation to attend things like MRCP teaching (unless you want to sit the exam) but all units have department teaching which you are expected to attend rota permitting and will boost your annual CPD points. It’s also a good chance to do a local presentation to colleagues or a Morbidity & Mortality review.
Year 2 – Getting your IAC, learning for the Primary FRCA and understanding critical care concepts.
Main Objectives:
- To transition from novice anaesthetist to having a basic understanding of anaesthetic principles and practises, developing practical airway and physiological management skills and handling emergency situations encountered in anaesthetic practise.
- To acquire the Initial Assessment of Competency (IAC) in Anaesthesia – this enables you to go onto on call rotas and be a bit more independent
- Start to gain knowledge to prepare for the primary FRCA
- Gain a foundation in critical care medicine, its evidence base and become more comfortable in managing level 2 and level 3 patients and organ support.
- Most importantly – don’t lose sight of your ACCS curriculum major and acute presentations sign-offs.
Expected Teaching to Attend:
- New Starter Anaesthetic Tutorials – For the first three months until you obtain your IAC. These are for anaesthetic trainees only as AM/EM have sessions for the “Non Anaesthetist”. They introduce you to the equipment, pharmacology, anatomy and physiology and record keeping that is expected of an anaesthetist and will support your day-to-day learning. Dates are on https://mmacc.uk/nw-anaesthesia/nwa-teaching under the heading “New Starter Tutorials” and are divided into North and South Schools. Again, these are virtual for now but you’ll be notified of the location when the pandemic subsides.
- Primary FRCA Tutorials – Half day tutorials again currently virtual covering different aspects of the Primary FRCA syllabus. Again, split into North and South Schools to make groups more manageable. https://mmacc.uk/nw-anaesthesia/nwa-teaching, under “Primary Tutorials”.
- Primary FRCA Regional Training Programme – These are separate to the half day tutorials and are often two days more intense study days on certain aspects of the curriculum. Not only are they full of information but outside of the pandemic help you network and meet up with colleagues and get into the primary FRCA exam mindset in practising questions and vivas. https://mmacc.uk/storage/Core%20Trainee%20Programme%20-%202020%20-%202022_26jan21.pdf
- Critical Incident Simulation Training – Forms part of the Anaesthesia regional training calendar and usually within six months of obtaining your IAC. These tackle anaesthesia specific scenarios such as failed intubation, anaphylaxis and malignant hyperpyrexia drills in teams and provide high fidelity simulation and reflective opportunities as well as a great chance for sign off of some of the major presentations in the ACCS curriculum.
- ACCS CT2 Decision Making Days – This is for the ACCS curriculum in general. Similar theme to the Critical Incident Simulation Training but less emphasis on anaesthetic emergencies. Again, excellent chance to complete DOPS/CEXs
- Intensive Care Medicine Study Day – Better placed in CT2 due to your 6-month block being in this year than in the final year of ACCS. Introduces you to some essential systems-based learning and organ support therapies that will also feature in the primary FRCA.
- Local Intensive Care Unit Teaching – Often very useful and can be journal clubs or topic based, excellent for CPD acquisition too or presenting a project.
Year 3 – Consolidating anaesthetic practise, gaining independence, obtaining the Primary FRCA, branching out into other areas. Readying for specialist applications
Main Objectives:
- To prepare for the primary FRCA – hopefully to pass but don’t be disheartened.
- Achieve the IAC Obstetric Anaesthesia
- Promote further independence with local supervision of anaesthetic practise as well as become fully integrated into the on-call rota.
- Compile a balanced CV and portfolio for specialist application (Anaesthetics and ICM)
- Enjoy a full year of anaesthesia with no specific commitments to AM/EM other than to complete any outstanding WBPAs.
Expected Teaching to Attend:
- Primary FRCA Tutorials – Half day tutorials again currently virtual covering different aspects of the Primary FRCA syllabus but acknowledging you may have been to some talks already in CT2 ACCS. https://mmacc.uk/nw-anaesthesia/nwa-teaching, under “Primary Tutorials”.
- Primary FRCA Regional Training Programme – These are separate to the half day tutorials and are often two days more intense study days on certain aspects of the curriculum. These days when face to face provide an excellent opportunity for exam practice with consultants and colleagues alike.
- Exam Practice Courses – There are separate dates for the MCQ and OSCE/Viva and are usually run a few weeks before a cycle of examinations. You need to register with Janet Coulson in advance of knowing when your exam will be. Also now an anatomy course that you can sign up to. https://mmacc.uk/storage/Core%20Trainee%20Programme%20-%202020%20-%202022_26jan21.pdf
- Other Study Days – Booked from the same link above
- Obstetric (Wythenshawe) – Introduction to obstetric anaesthesia and its challenges and anaesthetic techniques
- Airway – A great chance to learn about the assessment and management of difficult airways including some hands on experience with some fascinating and vital kit.
- Transfer Course – Essential in order to be accredited in the North West to do transfers. Simulates some scenarios, common emergencies and problems with inter-hospital transfers by ambulance as well as introducing you to the North West Transfer trolley setup.
- Medical Devices – An equipment training day that aims to standardise everybody’s knowledge and experience of various pieces of anaesthetic kit around the region, e.g. epidural pumps, infusions pumps, ventilators, etc.
Portfolio, ARCP and Maximising WBPAs
One major drawback of the ACCS system is that lifelong learning from the RCOA isn’t directly mapped to the curriculum, so there is a lot of improvisation that has to take place about uploading documents, namely in the CT1 year. However, if you speak to the college (training@rcoa.ac.uk) they should be able to add the curriculum on there for you.
There is an excellent guide on the ACCS homepage for the North West from one of the CT3 trainees: (https://nwpgmd.nhs.uk/sites/default/files/How%20to%20use%20Lifelong%20Learning%20for%20ACCS.pdf) but there are other ways of demonstrating your competency acquisition by keeping your own versions of logbooks. These can then emphasise which presentation or part of the curriculum each WBPA is mapped to and you can upload them as separate documents into Lifelong Learning afterwards.
Alternatively you can create larger PDFs with paper WBPAs attached to the logbook for the particular placement. The ARCP Checklists for ACCS are found here https://www.rcem.ac.uk/RCEM/Exams_Training/UK_Trainees/Assessment_Schedule.aspx?WebsiteKey=b3d6bb2a-abba-44ed-b758-467776a958cd&hkey=67d9cac9-8e51-4c86-b559-a1fa5c826530&Assessment_Schedule=2#Assessment_Schedule
The most useful approach is to periodically go back and check on your list of Core Major Presentations (CMPs) and Core Acute Presentations (CAPs) and think which placements are best suited for completing them:
Best Placements for Core Major Presentations (CMPs).
1. Anaphylaxis | Emergency Medicine |
2. Cardio-respiratory arrest | Acute Medicine |
3. Major trauma | Emergency Medicine |
4. Septic patient | Acute Medicine |
5. Shocked patient | Intensive Care Medicine |
6. Unconscious patient | Intensive Care Medicine |
Note these have to be CEX/CBD and by a consultant and have to be 2 per placement
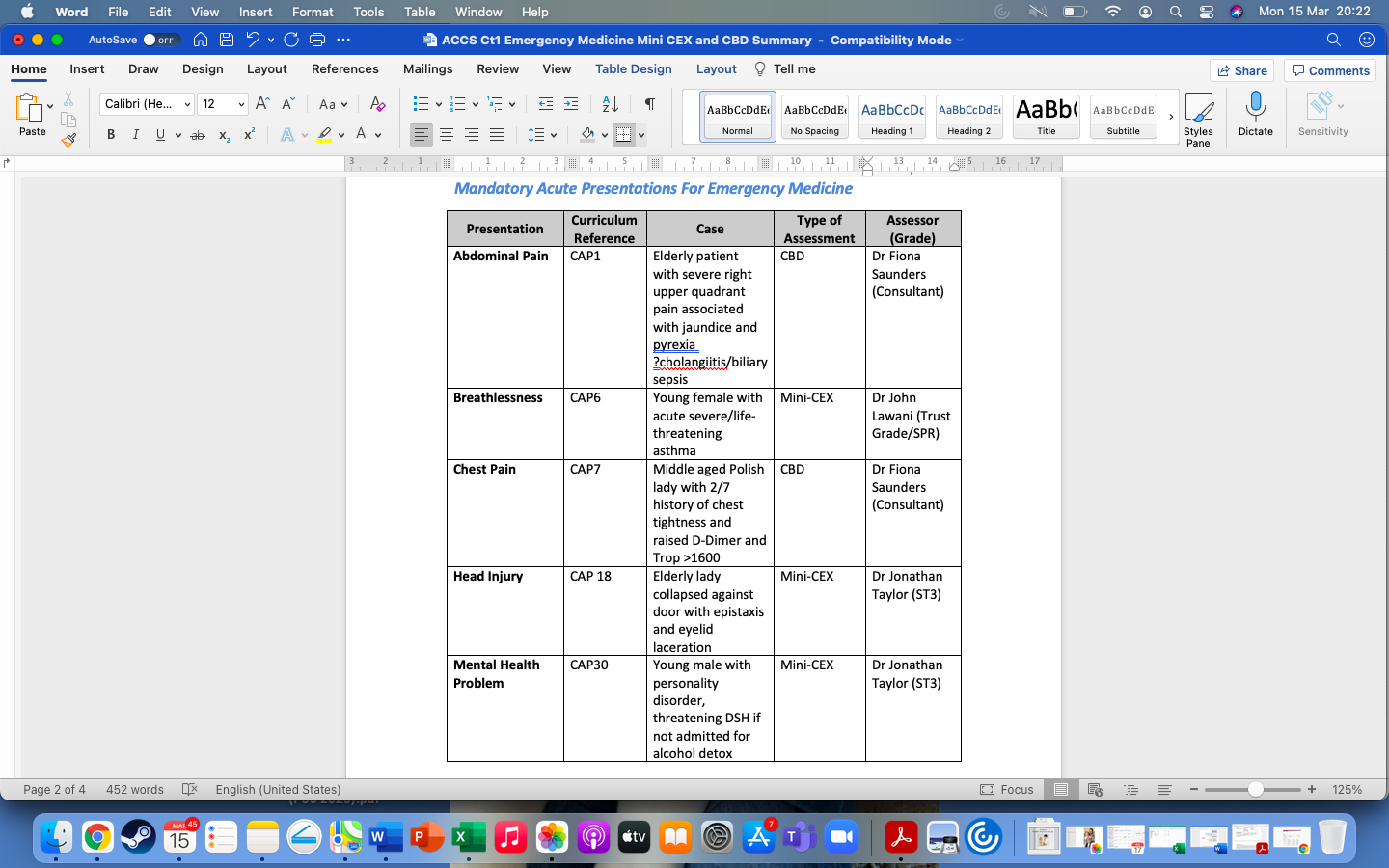
Best Placements for Core Acute Presentations (CAPs)

Practical Procedures During ACCS
The vast majority of these are straightforward to sign off and again it is a case of planning which placements are best for each assessments (see below). There are no “mandatory” assessments per placement, but for anaesthetics, the initial assessment of competency (IAC) components form a large part of the anaesthetic ones.


Sample Logbooks
Below are a few examples of the personal logbooks that you can keep and generate PDFs to upload to Lifelong Learning if your cases or procedures don’t fit the structure. They elaborate a bit more on your case involvement and can help provide evidence for any procedures you have done. I would also advise summarising the assessments you have completed against the checklist above.
Fig 1: Acute Medicine Example Case Logbook
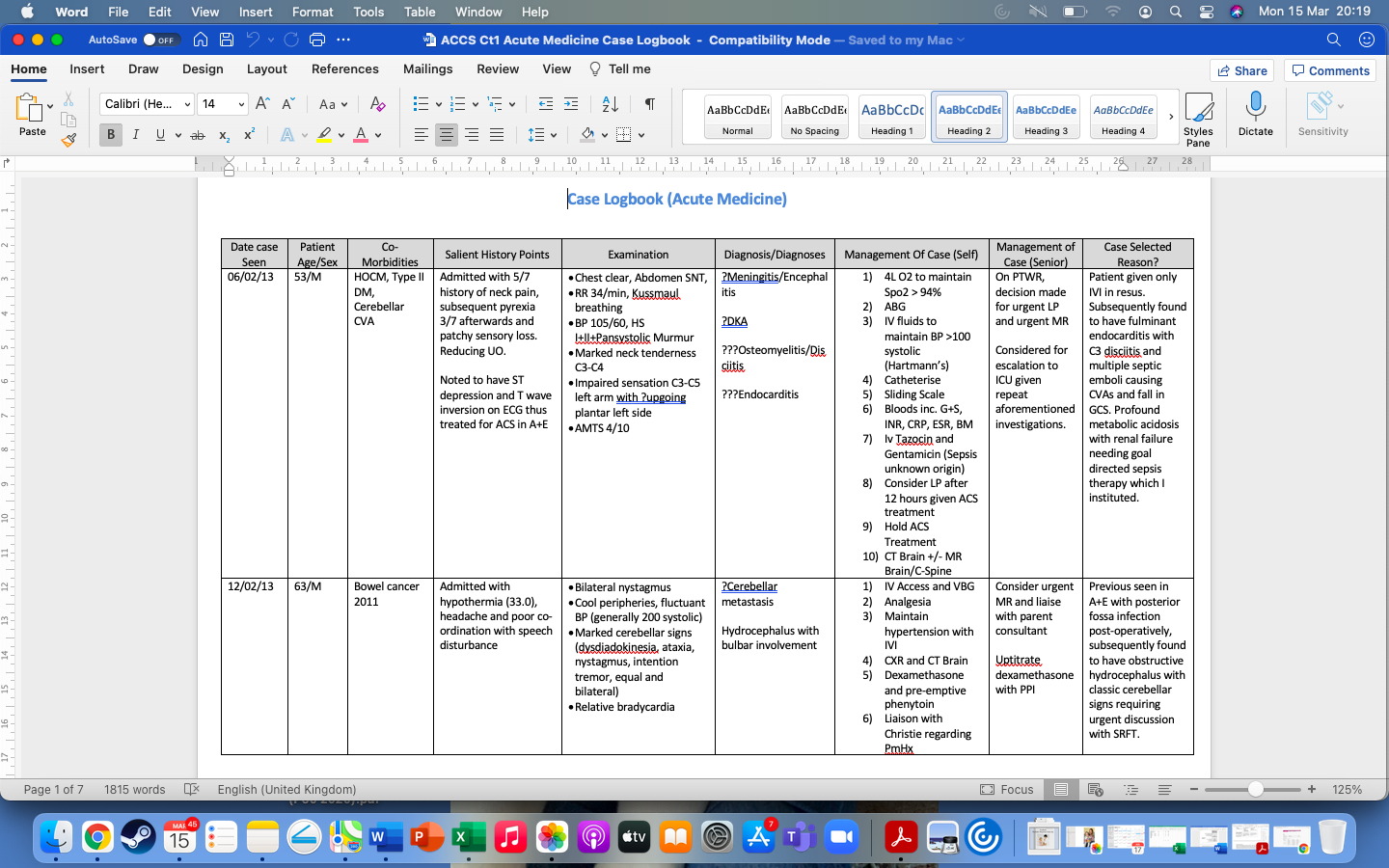
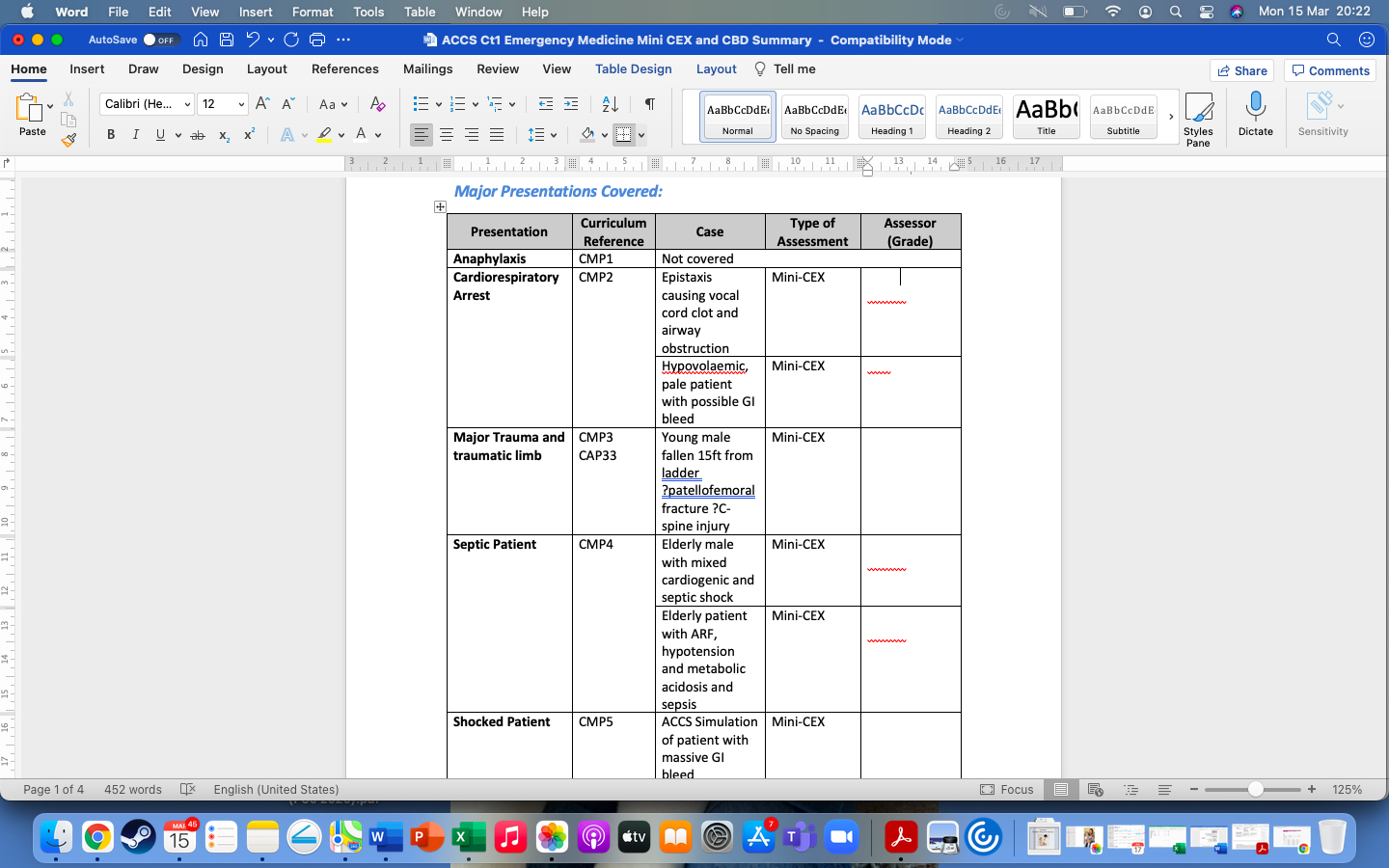
Fig 2: Emergency Medicine Summary of cases and curriculum coverage
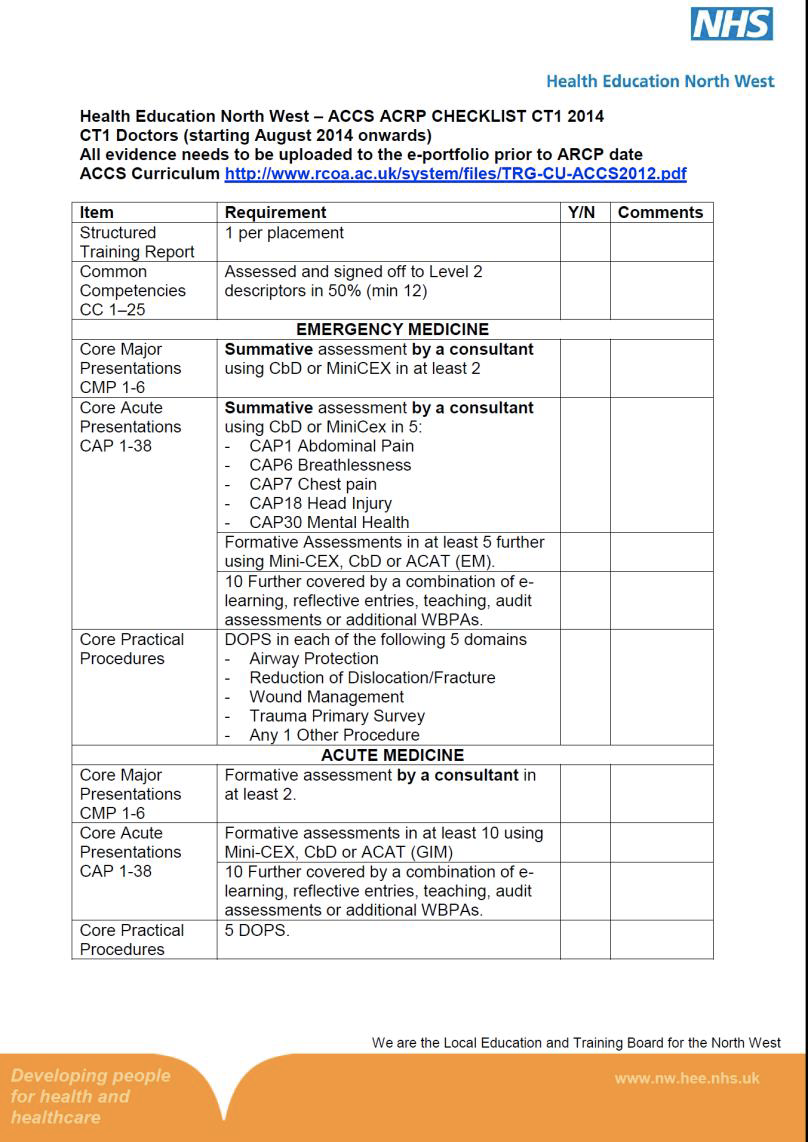
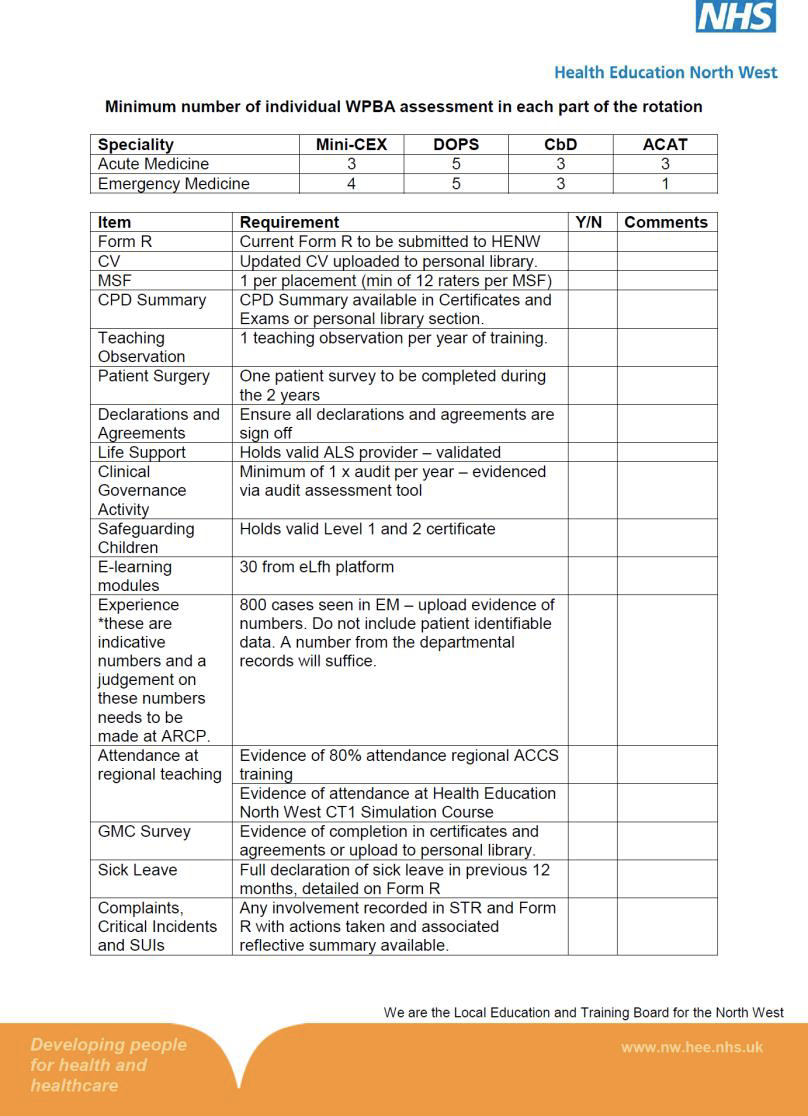
ACCS ARCP Checklist
This is the current curriculum and ARCP summary for each placement in ACCS: